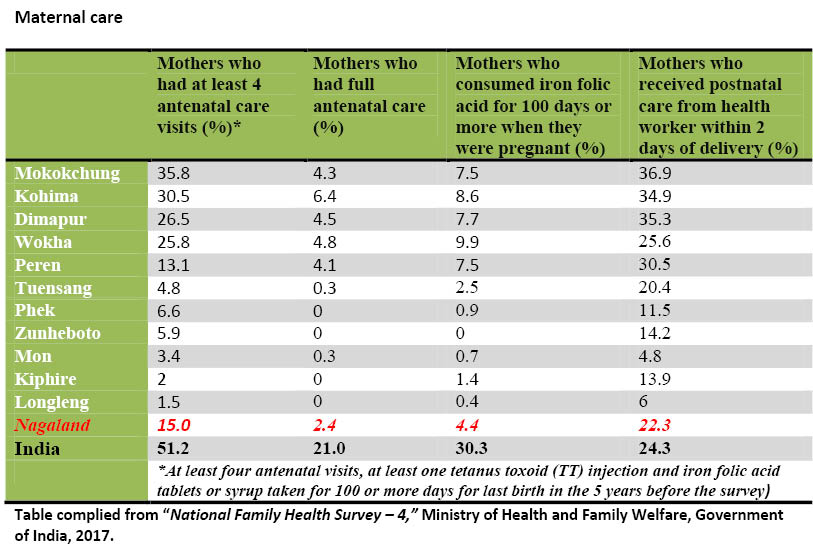
Table compiled from “National Family Health Survey – 4,” Ministry of Health and Family Welfare, Government of India, 2017.
Government critical to healthcare but underperforming
Moa Jamir
Dimapur | April 6
The overall status of maternity care and child immunization in Nagaland State is abysmally low, not even reaching half of India’s average on most indicators.
Within Nagaland, meanwhile, there are sharp regional disparities and the provision of healthcare remains highly skewed, calling for reorientation of priorities from all stakeholders.
An analysis of the recently released National Family Health Survey - 4 (NFHS-4; 2015-16) reveals district wise inequalities in health provision is staggering in Nagaland State.
Maternal and child care best in Mokokchung
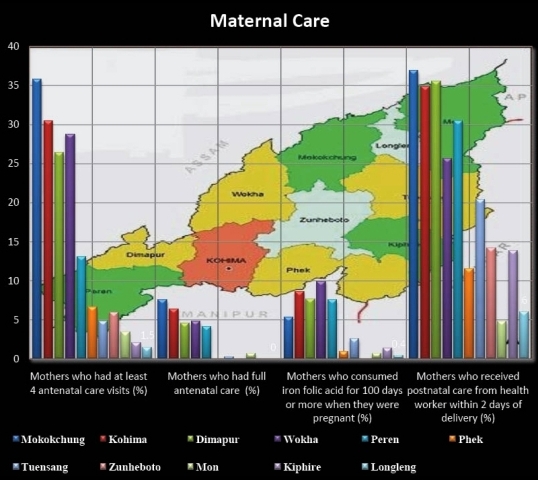
Though much below national average, according to the NFHS -4 data (see table), Mokokchung is the best performing district in maternal care followed by Kohima and Dimapur.
On the other end, Longleng has the lowest percentages in maternal care while the indicators in Zunheboto, Mon, Kiphire and Phek are also appallingly low.
In the case of child immunization and nutritional status, Mokokchung tops the indices, while Kohima and Peren closely follow. Full child immunization, however, is highest in Kohima. Five districts – Phek, Wokha, Zunheboto, Mon and Longleng — were below the State’s level in full immunization of children.
Sharp district wise disparities
The data shows huge district wise disparities in child and maternal care. For instance, if one looks at the percentage of mothers with at least four antenatal care visits (healthcare by professionals during pregnancy for last birth in five years before the survey), while top performing districts like Mokokchung and Kohima have 35.8% and 30.5% respectively, it is as low as 2% and 1.5 % in Kiphire and Longleng respectively, as per the NFHS-4.
In case of full antenatal care (at least four antenatal visits, at least one tetanus toxoid (TT) injection and iron folic acid tablets or syrup taken for 100 or more days), while almost all the districts have low averages, 4 districts shows zero visits, while in two others, it was below 1%.
The percentage for postnatal care of mothers from health professionals within 2 days of delivery also ranges from as high as 36.9% in Mokokchung to 4.8% in Mon.
Immunization – 5 districts below state’s level; all below national average
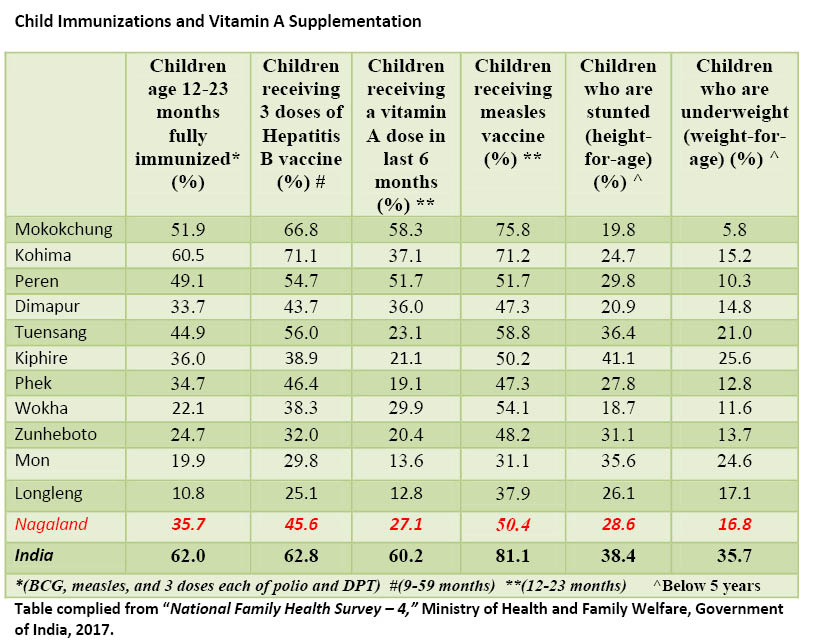
In case of full immunization (denoted by a BCG, measles, and 3 doses each of polio and DPT for Children aged 12-23 months), all the districts average below India’s 62% while five districts are below the State level of 35.7%.
However, district wise difference ranges from as high as 60.5% in Kohima to as low as 10.8% in Longleng. In case of children receiving three doses of Hepatitis B vaccine, the differences were 71.1% and 25.1%.
For children receiving vitamin A dose in last 6 months, 6 districts are below the State average of 27.1% while it was highest in Mokokchung at 58.3%.
Consequently, with lower nutritional intake, in five districts, children below 5 years who were considered ‘stunted’ - suffering from growth retardation as a result of poor diet or recurrent infections – are above the state level (28.6%) with Kiphire showing the highest incidence at 41.1%.
In case of underweight child below 5 years, four districts - Tuensang, Longleng, Mon and Kiphire have higher rate than the State level of 16.8%.
What disparities?
While the NFHS-4 data shows sharp disparities, how does one explains the outcome?
There is no clear explanation, however, an analysis of the district wise health units provided in the Nagaland Economic Survey 2006-17 and ctabulating the same with 2011 census could provide some answers.
In Dimapur and Kohima, for instance as per the Survey, a single government health unit is serving, on an average, 6210 and 4542 persons respectively. In Longleng this figure came to 4207, followed by Mon at 3475, Peren at 3400, Wokha at 3080, and Kiphire at 2551.
Beside geographical distances from the core, if we look at the access to health care in worst performing districts like Longleng, Kiphire, and Mon, almost 100% of the health care access is through the Government.
NFHS data showed that for almost all provision for immunization and other health care requirements, the public is dependent on the government.
Only Dimapur district had around 28% provision by private providers.
While the per unit density of healthcare for Dimapur and Kohima is relatively high, health provisions in these districts are amply augmented by private entities.
Such augmentations, however, are almost nil in low performing districts thereby leading to possible poor outcome.
Government critical to solve Nagaland’s Health Paradox
While Nagaland is above national average in most variables that contribute to infant mortality, the death rates are much lower than the former. Again, if one compares the average spending on health sector expenditure in Nagaland with other states, the health outcome does not commensurate with the expenditure.
Thus, heath care remains a paradox in Nagaland. For instance, spending a whopping Rs. 395 crore in, Nagaland State is sixth among Indian States on the list of per capita health expenditure (Rs 1707) and fifth on Health Expenditure as a percentage of Gross State Domestic Product (2.23%) in 2013-14 according to latest ‘National Health Profile 2016’ published by Central Bureau of Health Intelligence (CBHI).
By all accounts, with such expenses, it is expected that the State would score highly in both qualitative and quantitative delivery of healthcare to its citizens.
However, misplaced priorities as well as acute regional disparities seem to be pulling its health indicators down needing an urgent and critical course correction.